The Ethnomedical Approach
The ethnomedical approach to medical anthropology attempts to explain illness in relation to different populations. It focuses on the presence of different diseases among specific populations, but also looks at the different health systems of these populations as well. Anthropologists using this approach attempt to create explanatory models of health. They also look at the conditions of patients to seek treatment, how they are treated in the hospitals, and the methods of treatment used in the clinical settings.
The ethnomedical approach to medical anthropology is one of the areas that I am most interested in when it comes to studying Alzheimer’s disease. The concept of culture affects everything in our lives. It is our daily practices, our beliefs, our worldviews; our culture pretty much encompasses everything we are. So why, when treating our patients, do we not consider culture a factor when treating the illness?
In fact, certain cultures have lower rates of Alzheimer’s disease. Throughout my time at Michigan State University, I have focused my anthropology studies on Alzheimer’s disease and dementia and have actually done a lot of research on this particular phenomenon. The chart below shows the prevalence of Alzheimer’s disease among the three major races found in America:
The ethnomedical approach to medical anthropology is one of the areas that I am most interested in when it comes to studying Alzheimer’s disease. The concept of culture affects everything in our lives. It is our daily practices, our beliefs, our worldviews; our culture pretty much encompasses everything we are. So why, when treating our patients, do we not consider culture a factor when treating the illness?
In fact, certain cultures have lower rates of Alzheimer’s disease. Throughout my time at Michigan State University, I have focused my anthropology studies on Alzheimer’s disease and dementia and have actually done a lot of research on this particular phenomenon. The chart below shows the prevalence of Alzheimer’s disease among the three major races found in America:
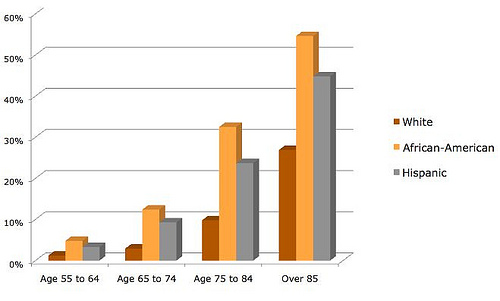
Image Credit: Big Think Editors
As you can see, White Americans show the highest occurrence of Alzheimer’s disease, followed by African-Americans, and lastly by Hispanic Americans. This higher prevalence may be caused by a number of things embedded in both the White American culture and also something that the Hispanic American culture presents as well. White American culture of the elderly people of our time was much different than the culture we now know and see today. Back when these aged people were growing up, they were raised to keep tight-lipped and to basically maintain your personal business as private. This is a huge factor that may not be realized when discussing this proportion. You see, while keeping their personal business private, many of the people who were raised this way, mainly White Americans of this generation, did not discuss openly their problems with memory loss and other early symptoms of Alzheimer’s disease, thus leaving it unrecognized. As it progressed, their symptoms became obviously outwardly apparent, and loved ones then had to take action and take them to be diagnosed and treated. But often this is too late for any preventative measures or effective treatments, and the patients die from Alzheimer’s disease.
The video below also demonstrates another way that culture may affect this ratio:
The video below also demonstrates another way that culture may affect this ratio:
Video Credit: VOA News
Studies have now shown that speaking a second language could delay Alzheimer’s disease. This is important to consider here, because many Hispanic Americans speak English, but also maintain their Spanish language as well. This very well could be a major influence in why the presence of Alzheimer’s disease is so low in Hispanic Americans.
It is important to understand that people in cultures other than our own deal with Alzheimer’s disease in a very different way than Americans do. Lawrence Cohen studied Alzheimer’s disease in India, and found very different ideas about Alzheimer’s disease than our own. You see, the Indian people view the aging process and the elderly body as sacred, quite the opposite of how Americans treat aging. They view those who are oldest to be the most valuable and important members of society, while Americans tend to view them as the lesser. Therefore, due to this cultural difference on the outlook on aging, many people in India do not see Alzheimer’s disease, nor any other aging disease for that matter, as a problem. It often goes undiagnosed and unreported. This is due to the fact that since these elderly people are viewed as such important members of society, the people of India do not see them being able to have such disease. In fact, the people of the four neighborhoods Cohen studied viewed memory lapses as "hot brain". "The centrality of "hot brain" - of anger rather than memory as a fundamental index of senile difference..." (Cohen) They view Alzheimer's disease as a temporary condition caused by anger, and not a disease caused by dementia. Alzheimer’s disease has the stigma of causing senility, and the elderly in India cannot possibly ever be viewed in this way.
One thing that is also very important to note here is that culture also effects how we treat Alzheimer’s patients. Alzheimer’s disease is a very personal disease due to the fact that it slowly effects the patient and it effects one of the most personal parts of the human body, the brain. Many different people of many different cultures view Alzheimer’s disease in various ways, and it is important to understand how the individual patient views their disease when treating them. Kleinman’s explanatory model of illness states the importance of understanding these differences. “Eliciting the patient’s (explanatory) model gives the physician knowledge of the beliefs the patient holds about his illness, the personal and social meaning he attaches to his disorder, his expectations about what will happen to him and what the doctor will do, and his own therapeutic goals.” (Kleinman) This is important to consider when treating this personal disease because different people may react differently to various treatments, making some more effective than others. For instance, while people in America may find biological medicine and professional treatments to be the most effective, the people in India may seek out folk treatments, or no treatments at all for that matter. Those in India would not find American medicine to be effective because the elderly only need their care, not a drug treatment.
Work Cited:
Big Think Editors. “Race, Gender, and Alzheimer’s Disease.” Big Think. November 19, 2010. Accessed July
24, 2013. http://bigthink.com/ideas/race-gender-and-alzheimers-disease
Cohen, Lawrence. "Toward an Anthropology of Senility: Anger, Weakness, and Alzheimer's in Banaras, India." Medical Anthropology Quarterly. Vol.
9, No. 3, pg. 314-334. September 1995. http://www.jstor.org/stable/649343
Kleinman, Arthur, Leon Eisenberg, and Byron Good. “Culture, Illness, and Care Clinical Lessons from
Anthropological and Cross-Cultural Research.” FOCUS 2006; 4: 140 – 149. Accessed July 24, 2013
http://focus.psychiatryonline.org/article.aspx?articleid=50511&RelatedWidgetArticles=true
VOA News. “Speaking 2nd Language Could Delay Alzheimer’s, Memory Loss” Video. March 15, 2011.
Accessed July 24, 2013. http://www.youtube.com/watch?v=DeVx68xGT0Q
It is important to understand that people in cultures other than our own deal with Alzheimer’s disease in a very different way than Americans do. Lawrence Cohen studied Alzheimer’s disease in India, and found very different ideas about Alzheimer’s disease than our own. You see, the Indian people view the aging process and the elderly body as sacred, quite the opposite of how Americans treat aging. They view those who are oldest to be the most valuable and important members of society, while Americans tend to view them as the lesser. Therefore, due to this cultural difference on the outlook on aging, many people in India do not see Alzheimer’s disease, nor any other aging disease for that matter, as a problem. It often goes undiagnosed and unreported. This is due to the fact that since these elderly people are viewed as such important members of society, the people of India do not see them being able to have such disease. In fact, the people of the four neighborhoods Cohen studied viewed memory lapses as "hot brain". "The centrality of "hot brain" - of anger rather than memory as a fundamental index of senile difference..." (Cohen) They view Alzheimer's disease as a temporary condition caused by anger, and not a disease caused by dementia. Alzheimer’s disease has the stigma of causing senility, and the elderly in India cannot possibly ever be viewed in this way.
One thing that is also very important to note here is that culture also effects how we treat Alzheimer’s patients. Alzheimer’s disease is a very personal disease due to the fact that it slowly effects the patient and it effects one of the most personal parts of the human body, the brain. Many different people of many different cultures view Alzheimer’s disease in various ways, and it is important to understand how the individual patient views their disease when treating them. Kleinman’s explanatory model of illness states the importance of understanding these differences. “Eliciting the patient’s (explanatory) model gives the physician knowledge of the beliefs the patient holds about his illness, the personal and social meaning he attaches to his disorder, his expectations about what will happen to him and what the doctor will do, and his own therapeutic goals.” (Kleinman) This is important to consider when treating this personal disease because different people may react differently to various treatments, making some more effective than others. For instance, while people in America may find biological medicine and professional treatments to be the most effective, the people in India may seek out folk treatments, or no treatments at all for that matter. Those in India would not find American medicine to be effective because the elderly only need their care, not a drug treatment.
Work Cited:
Big Think Editors. “Race, Gender, and Alzheimer’s Disease.” Big Think. November 19, 2010. Accessed July
24, 2013. http://bigthink.com/ideas/race-gender-and-alzheimers-disease
Cohen, Lawrence. "Toward an Anthropology of Senility: Anger, Weakness, and Alzheimer's in Banaras, India." Medical Anthropology Quarterly. Vol.
9, No. 3, pg. 314-334. September 1995. http://www.jstor.org/stable/649343
Kleinman, Arthur, Leon Eisenberg, and Byron Good. “Culture, Illness, and Care Clinical Lessons from
Anthropological and Cross-Cultural Research.” FOCUS 2006; 4: 140 – 149. Accessed July 24, 2013
http://focus.psychiatryonline.org/article.aspx?articleid=50511&RelatedWidgetArticles=true
VOA News. “Speaking 2nd Language Could Delay Alzheimer’s, Memory Loss” Video. March 15, 2011.
Accessed July 24, 2013. http://www.youtube.com/watch?v=DeVx68xGT0Q
